






Editor’s Note: Dr. Bennet Omalu, chief medical examiner of San Joaquin County, California, is an associate clinical professor of pathology at the University of California, Davis. His story is told in the new movie, “Concussion.” The opinions expressed in this commentary are his.
Story highlights
Dr. Bennet Omalu, whose story is told in the movie "Concussion," explains how he discovered the disease
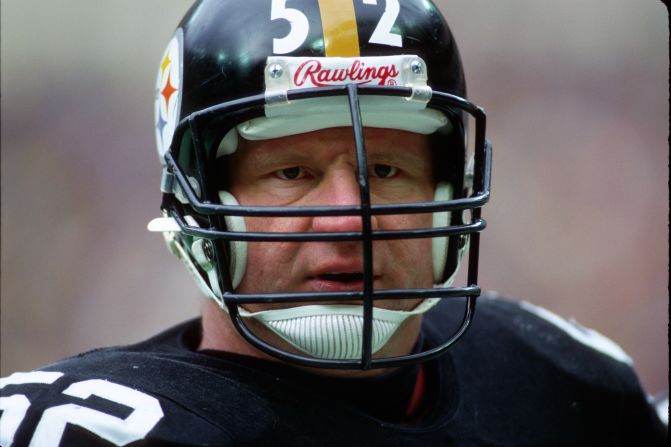
It began with an autopsy on the body of former Pittsburgh Steelers center Mike Webster
When I read Mike Webster’s file before I began his autopsy, I knew he was more than a 50-year-old heart attack victim. His file and the television reports of the death of the former Pittsburgh Steelers center described a long, steep fall into bizarre behavior. I suspected he suffered from some sort of brain disorder.
The potential diagnoses on my mind were post-traumatic encephalopathy (encephalopathy means brain disease, damage, or malfunction), Alzheimer’s disease, dementia pugilistica, aka punch drunk syndrome, and/or schizophrenia.

At this time there was no disease that I was aware of that was called chronic traumatic encephalopathy, or CTE. Dementia pugilistica was unlikely since he was not a boxer. Schizophrenia was unlikely since he did not have any diagnosis of that disease in the extensive pre-mortem clinical workup that he had. Alzheimer’s disease was less likely given his age.
Post-traumatic encephalopathy was about the only remaining diagnosis I had in mind while I performed the autopsy and considered the case. Based on what I knew about Webster’s career and his post-football behavior, I expected to see the residual damages of recurrent contusions and necrosis (death of body tissue), and even atrophy of a lobe in his brain, which would be characteristic of post-traumatic encephalopathy.
The story of the discovery of Webster’s brain disorder is worth telling, not only because of the upcoming release of the film “Concussion,” but also because some detractors have raised questions that I believe are unjustified.
No visible damage
I was flabbergasted when I opened his skull and saw a brain that appeared completely unremarkable without any visible damage. I saved his brain and fixed it in formalin because I was totally lost and confused by what I observed during the autopsy.
Could veterans have concussion-related CTE?
When I examined his brain and requested a battery of tests – histochemical and immunohistochemical stains – I honestly did not know what I was looking for, and I did not have any expectation of what I would see.

When I examined slides of Webster’s brain under a microscope I found abnormalities that I could not explain. The unique and distinctive topographic patterns of abnormal accumulations of proteins called tau and amyloid did not match with any neurodegenerative disease that I was aware of.
Because I had already excluded Alzheimer’s disease and dementia pugilistica, I was very surprised to see the abnormal accumulations of tau and amyloid in his brain, both of which occur in those diseases. Yet the topographic pattern, cellular architecture and distribution of these abnormal proteins were inconsistent with those diseases or any other of which I knew. I believed I had found something distinctive.
At this juncture, I wanted to show the slides to Dr. Ronald Hamilton, my professor and mentor who had taught me neurodegenerative diseases as a physician in training.
Seeking Hamilton’s opinion was consistent with the guidelines and standards of practice of pathology as has been established by the College of American Pathologists, that when you see something distinctive in a microscope, you may show it to a second pathologist to confirm the microscopic findings that you are observing. I took the slides to Hamilton, and he confirmed that I was not being delusional or hallucinatory: The microscopic findings in Webster’s brain were distinctive and unique.
Hamilton suggested that we show the slides of Webster’s brain to Dr. Steven Dekosky, the chairman of the University of Pittsburgh Medical Center Department of Neurology, and director of the Alzheimer’s Disease Research Center. Hamilton arranged the meeting. I went to Dekosky’s office and showed him the slides. He, too, confirmed that this was not Alzheimer’s disease and it was not dementia pugilistica. He agreed that I had observed a new syndrome and advised me to publish the paper of my findings. At this point we still had no clue what this new syndrome was.
A new disease
I went home and began a very comprehensive and extensive literature review to see if this observation had been published before in an American football player. I was utterly surprised that it had not.
Not a single paper had been published describing what I had observed in Webster’s brain. None whatsoever. I honestly could not, and did not believe it. It was simply impossible. Yes, much had been published on boxers, (the “punch drunk” condition known as dementia pugilistica) but nothing had been written on any American football player.
However, I did not want to report the paper simply as a case report describing the distinct pattern I had observed in Webster. I believed I had discovered a new disease in an American football player, a disease that had to be named. I did not know what name to give it, but I decided that whatever name I would give it would satisfy three criteria:
1. The name must be erudite and intellectually sophisticated.
2. The name must have a good acronym to facilitate recall should someone not be able to say the scientific name.
3. The name must be sufficiently generic, so that if someone down the road proved me wrong that this was not a distinctive disease, the name would still accurately describe the observed symptoms.

I am a forensic pathologist, and in the medico-legal consultations I had done, I had learned that precedent is very important in case law. This same principle applied to the acceptability of medical concepts in the court of law, frequently referred to as the Daubert rule or principle in the American judicial system.
If I derived a name that had been used in the literature as a descriptive terminology, took that descriptive terminology and converted it into a proper noun as the name of a disease, I was less likely to be deemed a radical, making my proposition more likely to be accepted by the medical community.
I therefore went back to the medical literature looking for descriptive terminologies that had been used to describe conditions resulting from primary brain injuries. In my research I identified and selected 24 descriptive terminologies that referred to long-term and delayed complications and outcomes of traumatic brain injury, but were not proper nouns of any specific disease with established pathology, especially in an American football player.
They are: cerebral neurasthenia, chronic traumatic brain injury, chronic brain injury, compensation hysteria, concussion neurosis, delayed traumatic apoplexy, dementia traumatica, encephalopathia traumatica, litigation neurosis, postconcussion neurosis, postconcussion syndrome, post-traumatic concussion state, post-traumatic head syndrome, post-traumatic psychoneurosis, terror neurosis, traumatic constitution, traumatic encephalitis, traumatic encephalopathy, traumatic encephalopathy of boxers, traumatic hysterias, traumatic insanity, traumatic neurosis, traumatic psychosis, and chronic traumatic encephalopathy.
Choosing a name
I spent days going through these names and analyzing them within the context of the three criteria I listed above. I finally settled upon two names:
1. Chronic traumatic brain injury
2. Chronic traumatic encephalopathy
Of the two, I preferred chronic traumatic encephalopathy. It accurately described what I found in Webster’s brain. Chronic means long-term, traumatic is associated with trauma, and encephalopathy refers to brain damage, disease or malfunction. The acronym, CTE, seemed easy to grasp and remember. The name sounded intellectually sophisticated. The name was sufficiently generic that if I were proven wrong and this was not a newly discovered brain disease, it still referred to a bad brain associated with trauma .

Chronic traumatic encephalopathy, or CTE, thus became the name of the disease I observed in Webster’s brain. Following DeKosky’s advice, I documented my findings in a paper entitled, “Chronic Traumatic Encephalopathy in a National Football League Player,” which was published in the journal Neurosurgery.
In the paper, which listed Hamilton and my boss, Dr. Cyril Wecht, as co-authors, I differentiated CTE as a distinctive disease, and presented the defining microscopic features in a case report defining Webster as a sentinel case. The paper indicated that other football players also suffered from the same disease. This is a very basic and fundamental step in epidemiological methods for the surveillance, identification and introduction of new diseases.
Before the case report on Webster, there was not a disease called chronic traumatic encephalopathy or CTE, although chronic traumatic encephalopathy had been used as a descriptive terminology in the literature. And this is why the National Institutes of Health recently published a paper for the diagnostic criteria for the pathologic diagnosis of CTE claiming that this was the very first time in history the pathologic criteria for the diagnosis of CTE were being published. If it was not a new disease, why would the NIH be publishing and presenting such criteria today?
Discovering more cases
Having published the sentinel case, I began searching for more cases in football players, because I believed a great majority, if not all professional football players, suffered from CTE. Discovering new cases was not difficult. Going by epidemiological methods, I published the second case of CTE in Terry Long, a football player and teammate of Webster, then a third in Andre Waters, a football player who played for the Philadelphia Eagles.
The third case qualified as a case series. I still searched for more cases of CTE in football players, and eventually published a cohort study. I identified and linked CTE with a distinctive constellation of presenting symptoms, which included suicidal behavior and suicides, which I also published.

I believed CTE existed in other high-impact contact sports athletes, and when Chris Benoit, a professional wrestler, committed suicide, I secured his brain and identified the first case of CTE in a wrestler. I again believed that some, if not all, the so called PTSD in military war veterans was a “blast variant” of CTE. Again I was the first to identify CTE in military war veterans. Moving forward, I believe CTE will become a disease that will have sub-types and variants.
Today, chronic traumatic encephalopathy has become a generally accepted disease and principle, if not common knowledge, in the medical literature. It has become a broadly diagnosed disease by clinicians and pathologists. In fact, I am very proud that some people have described the Webster autopsy as one of the most significant single events in the history of sports because of the discovery and diagnosis of CTE.
Knowledge of the disease spreads
Knowledge of the disease has now spread through all levels of football and society. Even my 8- and 6-year-old daughter and son, Ashly and Mark, know what CTE is. They may not be able to say chronic traumatic encephalopathy, but they can say CTE.
The search for the real cause of Webster’s death was, for me, a faith journey that epitomizes who we are as a common humanity. The search for this disease was not about gaining any sort of recognition for myself. Rather, I wanted to make a difference both for Mike and for all of us.
Some detractors, just like NFL doctors in the past, continue to deny that I discovered and named CTE when I performed an autopsy on Webster. These detractors continue to ridicule me like the NFL doctors have done. These insinuations are extremely hurtful and these are part of the reason I have always said that I wish I never met Mike Webster. I would never have imagined that 13 years after the Webster autopsy that certain people will still be making very calculated efforts to dehumanize, belittle, discredit and marginalize me and my work, just like it was 2002 all over again.
According to the Oxford Dictionary, to discover something means “to find (something or someone) unexpectedly or in the course of a search.” Therefore, just like Will Smith has said in the movie “Concussion,” “If you continue to deny my work, people will continue to die.” Anyone who continues to deny and misappropriate this work is dehumanizing Webster and the other athletes who guided me to the truth of the disease that ultimately contributed to their deaths.
It is my conviction that we are one love, one hope, one spirit and one body, bound together by the bond of peace. I wish us all every joy and happiness this Christmas, for that is actually what the movie “Concussion” is all about.
Join us on Facebook.com/CNNOpinion.
Read CNNOpinion’s Flipboard magazine.

