











Story highlights
The living brains of two ex-soldiers show damage similar to that of football players who have committed suicide
Brain trauma is a "signature injury" of wars in Iraq and Afghanistan
Chronic traumatic encephalopathy, or CTE, has no cure
After his last tour in Iraq, it took master gunner Shane Garcie about six weeks to notice he’d changed.
“Your brain is throwing parties because you’re home, you’re alive,” says Garcie. “So, it doesn’t settle in right away.”
Now he’s not sure what bothers him most: the fogginess of his brain, the anger that can erupt from nowhere or the deep, dark depressions he can’t shake off.
“One minute I’m in a good happy mood, everything is cool; the next minute I’m depressed,” Garcie told CNN chief medical correspondent Dr. Sanjay Gupta. “I don’t want to be around anybody, I want to isolate. Some days, I don’t want to get out of bed.”
“We could walk around this town and everybody, 90% of these people, would say, ‘Hey, Shane, hey,’ ” Garcie says about his hometown of Natchitoches, Louisiana. “But it’s not Shane. It looks like me, it walks like me, it talks like me, but it’s not me because of the damage.”
Since 1984, Green Beret Tommy Shoemaker has served in many war theaters – Kuwait, Iraq, Afghanistan, Somalia, Bosnia – and is still an Army reservist. He came home from Iraq to Monroe, Louisiana, in late 2006 with a bum leg and a disabled brain.
“I carry note cards and a pen with me everywhere I go, and when I’m talking to somebody, I write it down,” Shoemaker told Gupta. “Because if I don’t, I won’t remember. I mean memory was not a problem for me, I could remember anything. And now I have to write everything down.”
But it’s the mood swings he can’t control that do the most harm.
“I’ve always been really easygoing. Everything rolled off my back, no problems,” says Shoemaker in his Southern drawl.
“But now that’s not so. I mean, I’ll get mad over something as simple as a banana peel in the front yard or my wife saying the wrong thing to me, and is it really anything? No, but at that moment, it hits me and I just do things that I would’ve never done before. I yell, I scream, I holler, and that’s just never been my manner. I’m sad for my kids and my wife to have to live with that.”
“It’s tough, really tough,” agrees Pam Shoemaker, Tommy’s wife. “I do remember him telling me that ‘I’m different,’ ‘I’m not the same’” when he first came home. “I didn’t understand. But I do now.”
Brain studies
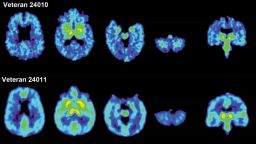
Dr. Julian Bailes, co-director of the NorthShore Neurological Institute in Evanston, Illinois, is pointing at the angry red and vivid yellow blooms on the PET scan of a living brain.
“Compared to normal controls, you see abnormal binding in the areas under the surface of the brain and deeper in the brain, showing abnormal accumulations of tau protein,” he explains.

All are signs of CTE, or chronic traumatic encephalopathy, a crippling neurological disorder caused by repeated blows to the head.
Characterized by deep depression, failing memory and anger that lurks just under the surface, CTE is a form of dementia that first came to light in the boxing world. “Punch drunk” was the term most often used for former pugilists, such as Muhammad Ali, who developed brain damage after a lifetime of hard knocks. Today it’s called dementia pugilistica and is considered a variant of CTE.
CTE is the disease many believe played a role in the deaths of former NFL players like Ray Easterling, Junior Seau, Shane Dronett and Dave Duerson. They all shot themselves. Duerson left a note asking that his brain be studied.
Images like these are traditionally gathered post-mortem, from brain samples taken at autopsy. That’s been the only way CTE could be diagnosed. Only a handful of studies have looked at living brains, with the hope a diagnosis could be made before death.
“Looking at living brains is a remarkable contribution to the science right now, a really remarkable contribution,” Dr. Geoffrey Ling told CNN. Ling is director of the Biological Technologies office at DARPA, the Defense Advanced Research Projects Agency. “It is very exciting and the potential is dramatic.”
In one of the largest studies of its kind to date, Bailes and his co-authors at UCLA compared the living brains of 14 former athletes thought to have CTE, 24 patients diagnosed with Alzheimer’s disease and two ex-soldiers, Tommy Shoemaker and Shane Garcie, to a control group of 28 cognitively normal people.
The researchers injected the participants with a radioactive “tracer” called [f-18]FDDNP before their PET scans. The tracer latches on to a brain protein called tau, which is thought to be responsible for much of the damage in Alzheimer’s and other degenerative brain disorders, and lights up areas of the brain that are affected.
“For us to be able to make the diagnosis of the injury or the disease in living people is paramount to being able to help them, treat them and to find some way to keep them out of progressing into a terminal problem,” says Bailes.
The scans of the ex-soldiers was a plus: a tiny sample designed to give a glimpse into what might be causing their debilitating symptoms.
And they offer a chance to explore what many experts are beginning to suspect: The blasts and energy jolts common in warfare might be creating a new form of CTE, a “blast-variant” version.
“In the military, it seems it would be vitally important to know who has been exposed to this, and then be able to identify, mark, follow the progression of brain degeneration from blast injury,” says Bailes. “And to know who’s at risk and maybe who needs to be pulled out of harm’s way permanently.”
Sure enough, the specific pattern of the tau the researchers found in Garcie and Shoemaker’s brains didn’t look at all like Alzheimer’s. Instead, it looked similar to the tau display found in the 14 players suspected of having CTE and the results taken from brain autopsies of people diagnosed with CTE.
Scan may detect signs of NFL players’ brain disease
And it looked similar to what had been found in a previous study by Bailes and his UCLA colleagues of the living brains of five NFL football players who were suspected of having CTE.
‘So many’ concussions
According to the Brain Trauma Foundation, 10% to 20% of Iraqi veterans are suffering from some level of traumatic brain disorder. The foundation even calls it the “signature injury” of the wars in Iraq and Afghanistan.
“One was a suicide bomber,” says Shoemaker. He’s recalling the last – and worst – of some 35 concussions he’s had over his military career. While about half of those rendered him unconscious, he says his training often took over.
“I was in an open vehicle with no top between me and the explosion. So I had some shrapnel and suffered a concussion, but I was able to stay focused enough with muscle memory to just keep driving, ‘til my head kind of cleared, and I kept going.”
“And the other one was a roadside bomb. I was knocked unconscious but again was able to just out of memory continue driving, not even realizing what had happened.”
Shane Garcie can’t recall how many concussions he’s had.
“No, because there’s so many. There’s so many,” says Garcie. “There are so many reasons for the jarrings, for the beatings. Not just IEDs, not just car bombs, not just in a firefight or grenades going off.”
“Think about it, you know. Iraq doesn’t have the best roads,” Garcie continues. “And you hit that bump and your head – it smacks the turret. Rollovers are severe because of the canals. I mean, you’re driving in blackout mode on dark nights, with nods on and no lights – you can barely see 10 feet in front of you. There are so many ways it can happen.”
New form of dementia?
The science of CTE is in its infancy. A band of researchers around the country has been racing to catalog as much information as possible, to answer the questions: Is CTE distinct enough to be diagnosed? Is it a “new” neurodegenerative disease?
“Before people run out and say, ‘Oh, this person has CTE, or that person has CTE,’ I think that’d be way premature to do that,” says Ling. “Chronic traumatic encephalopathy, that’s a condition that still needs further study.”
Researchers struggle with how to tease out the differences between post-concussion syndrome, a chronic but stable disease, and CTE, which early research shows spreads from the initial site of impact throughout the brain and worsens with age.
“There’s so many things about CTE we don’t understand,” says Bailes. “There never has been long-term longitudinal studies that analyze who gets it and exactly why, what the prevalence of it is, and then who progresses. There may be a group that doesn’t progress.”
The type of radioactive marker to use, and how accurate it is in binding to tau protein, is also under scrutiny. A number of tau trackers are in the works, and each seem to have unique characteristics. The UCLA study’s [f-18]FDDNP is an older marker that critics say isn’t specific enough because it can also bind to amyloids, which are misfolded proteins commonly seen in Alzheimer’s brains.
Bailes defends [f-18]FDDNP this way: “Most CTE sufferers have been found at autopsy to have tau, but also about 40% have had amyloid as well. So they are showing both degeneration markers in the brain,” says Bailes.
“Most importantly, it’s a distinct pattern that we haven’t seen in any other condition – not in Alzheimer’s, not in other forms of dementia, and certainly not in normal controls. So it’s not just what we’re binding to, it’s that this pattern appears to be distinct and it appears to be the areas that have been damaged in autopsy studies of sufferers with CTE.”
Ling has a more global view. “In the end, these scans are just scans. That’s all that they are. It really has to do with the context of the patient. We have to understand the patient: What is their history? Do they have multiple head injuries? Do they have anything else that could compound this?”
Several of the study’s co-authors, including Dr. Gary Small; Jorge Barrio, Ph.D.; Dr. Bennet Omalu and lawyer Robert Fitzsimmons, have licensed [f-18]FDDNP from UCLA and created a company named TauMark to develop the tracer. Bailes is not affiliated. In February, the FDA warned TauMark not to promote [f-18[FDDNP out of concern it was overselling a not yet proven or tested diagnosis tool. The company has since downplayed the language on its website.
Right now, prevention is the only treatment
At this time, there is no cure for CTE. There are no real treatments, either. All that can be done is to treat the symptoms. Psychotherapy and antidepressants are often prescribed for anxiety and anger, while memory issues are tackled with lifestyle and diet changes that may or may not help.
“There really is no concussion pill, there’s no specific medication we have to treat these,” says Bailes. “It’s recognition, it’s taking that individual out of harm’s way for future impacts or blast injury, and it’s allowing the brain to heal.”
Experts agree that accurately identifying brain injury on the spot is critical. That’s because the risk increases each time you have one. “Every concussion predisposes you to be a little more sensitive to have another one, especially if they are in close proximity time wise,” says Bailes.
The hope is that science will develop a test that can diagnose brain trauma in war zones or on the sidelines of a football game at the time of injury. Several are in development, but only a pencil-and-paper test is in use right now.
For Shane Garcie, all that matters is what can be done to keep other soldiers from ending up like him.
“I’ve talked to other doctors and a couple of neurologists and neurosurgeons, and they’re like, ‘Man, really, I don’t know how you’re functioning like you are,’ he says. “I could’ve been a comedian. I was very quick-witted, very smart. Now I stutter. I sputter. I lose words. I can be having a conversation and forget everything we’re talking about.”
“But it’s not just Shane that’s having all these brain issues. There were thousands of troops who were getting blasted by IEDs, car bombs, RPGs, grenades. I want them to know that they’re not alone.”
For Tommy Shoemaker, it’s important that soldiers with CTE receive a physical diagnosis, rather than just being lumped under the umbrella of post-traumatic stress disorder. To him, it matters a great deal that his symptoms are the result of a brain injury, instead of the inability to cope with the emotional fallout of trauma.
“People are more apt to accept a physical disorder than they are mental disorders,” he says. “So if you can do that for soldiers, I think that’s a big plus.”
“I think it’s a plus when they go to get a job, you know, and they ask ‘em: ‘Do you have a mental disorder?’ Well no, I don’t. I have a brain injury. Nobody wants to be diagnosed as having a mental disorder.”

